nt 动漫
你的位置:
萝莉少女 >
nt 动漫 > av 巨屌 Re:【原文发布】《柳叶刀》6月份综述:脑卒中的弥留救治与长久方分(已认领123
av 巨屌 Re:【原文发布】《柳叶刀》6月份综述:脑卒中的弥留救治与长久方分(已认领123
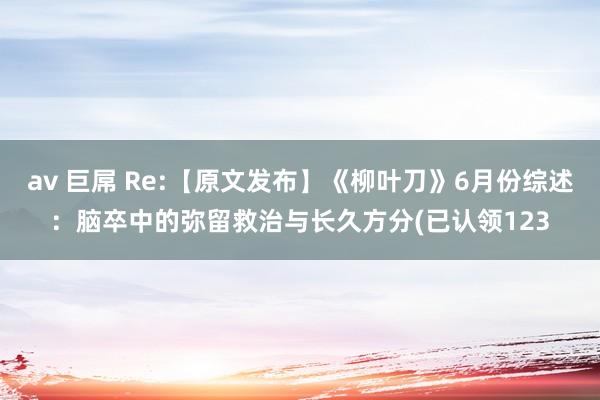
发布日期:2024-08-26 04:06 点击次数:142
RESOURCE: The Lancet Neurology, Current Issue, Volume 6, Number 6, June 2007 /Lancet Neurology 2007; 6:553-561DOI:10.1016/S1474-4422(07)70005-4全文分八部分,请诸君战友认领翻译校对TITLE: Acute treatment and long-term management of stroke in developing countriesAUTHOR: Prof Michael Brainin MD , Yvonne Teuschl PhD and Lalit Kalra MD第一部分SummaryDeveloping countries have some of the highest stroke mortality rates in the world that account for over two-thirds of stroke deaths worldwide. Hospital-based studies suggest that the patterns of stroke types and causes of stroke differ between developing and developed countries, resulting in differing needs for acute and long-term care. Data on stroke care provision in developing countries are sparse and most of the available studies are biased towards urban settings in reasonably resourced health-care systems. A general overview shows that the quality and quantity of stroke care is largely patchy in low-income and middle-income countries, with areas of excellence intermixed with areas of severe need, depending upon patients' location, socioeconomic status, education, and cultural beliefs. Here we review the available literature on acute and long-term stroke management in developing countries. On the basis of available studies, largely from developed countries, we discuss the need to develop basic organised stroke-unit care in developing countries.IntroductionStroke is the second commonest cause of mortality worldwide1 and remains a leading cause of adult physical disability. Developments in stroke care over the past two decades, particularly in acute management as well as in rehabilitation and long-term care, have greatly reduced mortality and dependence in many developed countries. Indeed, 10 year stroke mortality rates collected by the WHO MONICA project in Europe and China showed that changes in mortality rates in nine countries were mainly due to changes in case fatality rather than to changes in stroke incidence, suggesting that changes in the quality of stroke care may be responsible for changes in stroke mortality.2,3 By contrast, there has been limited progress in the management of patients with stroke in developing countries, despite increasing incidence of stroke and high stroke mortality rates that account for over two-thirds of stroke deaths worldwide.4 The slow uptake of evidence into clinical practice can be attributed to several reasons mainly relating to geography, limited health-care provision for the population as a whole, socioeconomic considerations, and health behaviour of different populations. In addition, hospital-based studies suggest differences in the type and causes of stroke between developed and developing countries, with higher incidence of haemorrhagic stroke and higher prevalence of stroke due to infective or inflammatory causes. Although many of the advances associated with reduced stroke mortality and morbidity will be equally applicable to developing countries, differences in types and causes of stroke, limitations posed by geography, accessibility of health care, availability of resources, social beliefs, and cultural expectations need to be taken into account when extrapolating stroke-management strategies from the developed to developing countries.5第二部分Specific issues in the treatment of stroke in developing countriesResearch on stroke-care provision in developing countries is sparse and most of the available studies are biased towards urban settings in affluent economies with reasonably resourced health-care systems. A general overview shows that the quality and quantity of stroke care is largely patchy in low-income and middle-income countries (or low-developed and medium-developed as defined by the United Nations Development Program6), with areas of excellence intermixed with areas of severe need depending upon location, socioeconomic status, education, and cultural beliefs.Stroke awareness and use of hospitalsThe importance of stroke awareness has been highlighted in many studies, which show poor recognition of stroke symptoms in developing countries. Only one in 25 patients attending a stroke clinic and 27% of patients presenting to the stroke services in a tertiary hospital in India were aware that they had suffered a stroke.7,8 Equally importantly, 80% of the patients in the first study thought that the organ affected was the heart and only 33% of patients in the tertiary hospital setting knew that the brain was involved in stroke. Moreover, 29% of patients with stroke in the second study did not know a single warning sign. However, in another study in the same hospital in India, 55% of the relatives of patients without history of stroke identified the brain as the affected organ, and only 23% could not cite a single stroke symptom.9 A study in a university hospital in Oman found that 35% of patients with high risk of stroke stated that the organ affected by a stroke is the brain and 68% identified at least one stroke symptom.10 However, stroke awareness and knowledge is poor even in developed countries and varies as in developing countries9,10 with income, education, age, and sex.11–15 The proportion of people correctly identifying the brain as the organ involved in stroke in developed countries was between 45% and 73%,11,12,15,16 and between 30% and 90% knew at least one stroke warning sign.11–18The multiplicity of health-care options, many of which may not be rooted in biological sciences, may be a significant impediment to early intervention in patients with acute stroke. In an Indian study in an urban setting, 59% of patients with stroke consulted a private doctor before seeking hospital care and only 38% of patients presented directly to hospital.8 Studies in rural South Africa show that 40–80% of patients complement medical care with help from traditional healers or churches and as many as 10–33% of patients may go to traditional healers first rather than seek medical help.19,20 The rural–urban split in access to stroke treatment is also reflected in studies from Taiwan and Bolivia, which show that 10% and 50%, respectively, of patients with stroke in rural settings do not go to hospital or see a doctor.21,22 Hospital is the first point of investigation and treatment for many patients. Overall, the proportion of patients with incident stroke who present to hospitals in poorly developed or moderately developed countries is difficult to estimate. A hospital-based study from the Philippines suggests 81% of patients present at hospitals;23 whereas a prospective population study from the Ukraine showed that 66% were hospitalised.24 These estimates are derived from regions with reasonably well-developed health services and may not be representative of other developing countries.第三部分Thrombolysis and hospital careIn developing countries, there is great variation in the time taken by patients with stroke to present to hospitals and the imaging or treatment facilities available for their management (table 1).23,25–35 Most studies suggest that patients with stroke who present to hospital, do so fairly soon after symptom onset. Studies from The Gambia show that most patients were admitted within 48 h of symptom onset,26 the median time to admission being 8 h.25 A study from Ethiopia reported a median time of 13·5 h before presenting to hospital.36 Studies from urban hospitals in India and the Philippines report that up to 35% of patients with stroke present within 3 h of symptom onset,8,23,30 which is no different to the times to presentation reported from developed countries.37Table 1. Acute management of stroke in developing countriesThe use of imaging also differs considerably between settings (table 1). In 1998, 18 African countries had no CT scanners and 13 countries had one each. Only northern African countries and South Africa had an appropriate number of CT and some MRI scanners.38 CT scanning facilities were not available in 27% of hospitals in the Philippines,23 but 83% patients with stroke in a general hospital in China had either CT (65%) or MRI (43%) scans.29 In 1998, Shanghai (China) and Malaysia had about one or two MRI scanners per million population whereas in Thailand, the Indian state Tamil Nadu, Indonesia, and the Philippines fewer than 0·5 scanners per million population were available.39The reported rates for thrombolysis also vary substantially, ranging from 2·1% in a large study in 1624 patients in Thailand32 to 7% in a smaller study of 489 patients from India.31 Intravenous alteplase (recombinant tissue plasminogen activator; rtPA) is registered and introduced in many countries with medium development and some with low levels of development. Affordability was an important determinant of both investigations and treatment in some settings: only 101 of 1102 (9%) patients with stroke in Nigeria could afford to have CT scans;40 in Ethiopia, CT scan was only done in 38·3% of patients due to its high price;41 and 10% of 489 patients with incident stroke who meet all criteria for thrombolysis were not given the treatment in an Indian study because they could not afford alteplase.31The length of hospital stay varied substantially according to region and affordability. The median hospital stay in Pakistan was only 3 days,35 compared with 32 days for insured patients in China.29 There is very little information on specialised stroke-unit care in developing countries. A study from Brazil showed no differences in outcome measured at 10 days after stroke onset or length of hospital stay between those managed on a stroke unit and those on general wards.34 However, there was a trend towards lower mortality at 1 month, 3 months, and 6 months in patients managed on the stroke unit, which did not achieve statistical significance, possibly because of the small sample size. Another study from Thailand that compared hospital care with hospitalisation and early supported discharge showed no differences in mortality but better patient perceptions of the care received in those managed at home.33第四部分Access to and availability of adequate rehabilitation facilities is also limited in countries with low or medium development. Only 47% of hospitalised patients with stroke were seen by a therapist in The Gambia;26 and in large teaching hospitals in southern China, routine care included no regular professional physiotherapy during the whole hospitalisation period.42 The mean duration between stroke onset and admission to a rehabilitation facility is 53 days in Thailand and 63 days and 76 days in two Turkish studies.43–45 In South Africa, only 39% of old and 56% of young patients with stroke attended outpatients' physiotherapy clinics once a week or once a month after hospital discharge.46Secondary preventionMost studies show poor outcomes in patients with stroke in terms of mortality and implementation of secondary prevention measures (table 2).19,25,26,33,34,42–51 Many of the problems of poor concordance with secondary prevention measures have been attributed to lack of equipment for the monitoring of blood pressure or other risk factors, non-availability of drugs, and affordability of treatment.19,50 A Chinese study showed that lower socioeconomic status was associated with higher 3 year mortality in patients with ischaemic stroke.49 Cost-effective secondary prevention has been proposed by WHO guidelines for low-income and middle-income populations, suggesting lifestyle changes and affordable, accessible, and effective pharmacological antihypertensive treatments, antiplatelet treatments, and blood-cholesterol reduction.52 Aspirin has been recommended as the most cost-effective antiplatelet medical therapy worldwide because it is cheap and easily available everywhere in the world but compliance with treatment is commonly poor.52–54 Studies from The Gambia26 and South Africa19 reported that although 65% and 83% respectively of stroke patients were treated with antihypertensive drugs at the time of discharge, only 13% of stroke survivors in The Gambia and 8% of survivors in South Africa were taking antihypertensive treatment after 1 year. Similarly, of the 71% of patients discharged on aspirin in The Gambia, only 7% were still taking aspirin 1 year later.26 In another study from The Gambia, 33% of stroke survivors were treated with antihypertensive medication at 6 months after stroke; 3–4 years later only 15% were satisfactorily controlled for hypertension and 15% received aspirin regularly.25 The WHO PREMISE study of ten medium developed countries (Brazil, Egypt, India, Indonesia, Islamic Republic of Iran, Pakistan, Russian Federation, Sri Lanka, Tunisia, and Turkey) reported high percentages of patients with cerebrovascular diseases using drugs for secondary prevention. Aspirin use ranged from 31% to 90%, the use of beta-blockers from 6·8% to 46%, angiotensin-converting-enzyme inhibitor use from 5% to 59%, and statin use from 2% to 37%.50 94% of these patients reported that their blood pressure had been measured within the past 12 months. Patients in this study were recruited from outpatient clinics, which may reflect better access to health services and greater acceptance of drug treatment than among the general population in these settings.Table 2. Long-term management of stroke in developing countries第五部分Little information is available on lifestyle modification after stroke in developing countries. The PREMISE study suggests that 77–89% of patients have knowledge of the benefits of smoking cessation, diet modification, and regular physical activity. However, 52·5% did not engage in regular moderate physical activity, and 35% had difficulties in complying with dietary advice due to the expense and lack of availability of healthy food items.50 On the Kinmen islands, China, 36% of stroke survivors eat meat less than once per week and 36% exercise more than once per week compared with 19% and 18% respectively for people who had not had stroke.21 The figure shows the location of the studies covered in this Review.Figure. Locations of the studies covered by this reviewPurple circles indicate studies reporting data on stroke care in the strict sense; yellow circles indicate studies reporting data on additional care-relevant subjects according to high (green), medium (blue) and low (red) human development based on the Human development report 2005.1Differences in stroke type and causeRecent systematic reviews of population-based studies show only moderate geographical variations in stroke incidence in the world.55 Most of the stroke incidence in developing countries is likely accounted for by the increasing prevalence of conventional risk factors such as hypertension, diabetes, hypercholesterolaemia, and smoking as populations adopt a more urbanised lifestyle. However, there are some important differences in stroke type and cause between developed and developing countries, which become important from a management perspective. Many hospital-based studies suggest a significantly high proportion of stroke patients have intracranial haemorrhage, the proportion varying between 19–60% in various studies.23,26,40,41,47,48,56–61 However, hospital-based studies are likely to be biased towards the more severe end of the stroke spectrum in developing countries because of factors such as distance from hospital, access to transport, ability to afford hospital fees, and local beliefs about hospital attendance, which reduce rates of hospitalisation for patients with mild stroke. There are very few community-based studies in these settings and, therefore, a paucity of reliable data on stroke subtype prevalence in developing countries.第六部分Uncontrolled and commonly undiagnosed hypertension remains the most important cause of intracerebral haemorrhage in developing countries, but a high proportion is attributable to aneurysms and arteriovenous malformations.28,62 Although the prevalence of atherosclerotic and cardioembolic stroke seems to be the same in developing and developed countries, cardioembolic strokes occur at a younger age and are more commonly caused by valvular involvement in rheumatic or congenital heart disease in developing countries;62,63 there is also a higher prevalence of strokes caused by sickle-cell disease, vasculitis due to infection, or inflammation and coagulopathies (table 3).64,65Table 3. Causes of stroke specific to developing countries65Implementing evidence-based management in developing countriesA major development over the past decade has been the setting up of specialised stroke centres in many developed countries to provide early thrombolysis and clot removal therapy for acute patients with ischaemic stroke, on the basis of the principle that “time is brain”.66,67 The approval and licensing of thrombolytic therapy for ischaemic stroke in North America and Europe has helped to spread the practice of specialised stroke care from tertiary academic centres to large networks of acute stroke units in local hospitals and the emergence of guidelines for the management of acute stroke.68,69 There are now precise North American and European definitions of the organisation of acute stroke centres that take into account the range of interventions and imaging facilities.67,70 While large tertiary academic centres may offer a range of highly specialised therapy options—such as interventional neuroradiological and neurosurgical therapies, including the technical set-up for intra-arterial thrombolysis, haematoma evacuation, hemispheric craniotomy, and carotid surgery—local stroke units in regional hospitals may offer a smaller, less costly, but nevertheless effective service including rapid diagnosis assisted by CT imaging; intravenous thrombolysis in eligible patients; acute stroke care to maintain physiological homoeostasis and prevent stroke-related complications; management of dysphagia, nutrition, and communication; early mobilisation; and therapy for sensorimotor and cognitive impairments. Despite limited access to highly specialised procedures, local centres have the potential to deal with most strokes and stroke-related complications and selected patients need to be transferred to large centres only rarely.第七部分The mainstay of management in any setting, whether a highly specialised tertiary stroke centre or a low-level local stroke unit, is a structured approach towards patients with acute stroke and their continuous management in the postacute phase by dedicated staff trained to recognise, monitor, and treat stroke-related problems.71 There is general consensus among stroke specialists that the most effective components of acute stroke that improve overall outcomes consist of rapid and precise diagnosis, proactive general measures for prevention, and early recognition of complications and early mobilisation.72 Hankey and Warlow have extrapolated data from randomised studies to efficiency measures with a population-based approach and shown that the benefits of treatment in stroke units are much greater than those of treatment with intravenous thrombolysis.73 This is because the proportion of patients likely to be treated in stroke units is much greater than that treated with thrombolysis at present.Many developing countries have stroke centres that can provide imaging and interventional facilities comparable to major academic centres in developed countries. However, a high rate of thrombolysis does not reflect the overall quality of stroke care, but only represents a good prehospital setup and an effective rapid response to stroke presenting as an emergency. Although thrombolysis may result in significant improvements for individual patients, its effectiveness as an intervention to improve population outcomes is likely to be diluted because of its limited use in highly selected patients presenting early to specialist centres. The highest priority for providers of a stroke service in less well organised or less affluent settings must be to establish a stroke unit and multidisciplinary team to deliver organised stroke care.73 This approach has been widely adopted in developed countries, where the bulk of stroke care is provided by networks of local stroke units. Countries with low and medium levels of development might be best off aiming for a stepwise development of specialist stroke services, which favours the establishment of a basic stroke unit before setting up specialised teams for thrombolysis. This is particularly important because a higher proportion of patients in developing countries have haemorrhagic stroke and it may be difficult to implement sophisticated management paradigms for time-dependent interventions in patients with ischaemic stroke because of inadequate prehospital facilities and unreliable transportation.第八部分Specialised stroke units are an ideal opportunity for education and information on stroke prevention to patients and their families. Studies have shown that patients provided with structured information on measures to prevent further strokes in such settings have the highest adherence to long-term medication and lifestyle changes after stroke in developed countries.74 Non-compliance for long-term treatment—even for aspirin—is relatively high in developing countries. Education on behavioural modification and medical therapies during hospitalisation by specialists using simple messages adapted to patients' education and cultural background may be an opportunity to increase adherence to secondary prevention measures. The family has an important role in developing countries and should be included in health education to encourage and help patients with drug intake and lifestyle changes.ConclusionsDeveloping countries have some of the highest stroke mortality rates in the world that comprise over two-thirds of stroke deaths worldwide. Patterns of stroke types and causes of stroke differ between developing and developed countries but there are few studies of acute stroke care or long-term management to guide clinical practice. The quality and quantity of stroke care is patchy in developing countries, with areas of excellence intermixed with areas of severe need depending upon patients' location, local hospital facilities, ability to pay, education, and cultural, social, or religious beliefs. A population-based approach to improving acute care and rehabilitation for stroke is needed, which is evidence based and maximises the effectiveness of such care. Existing literature, largely from developed countries, supports the development of basic organised stroke-unit care, which must be tailored by health needs, service patterns, and affordability of individual settings. Further research is also needed to develop customised acute care and rehabilitation strategies most appropriate to the needs and circumstances of developing countries to help them alleviate the growing burden of stroke.第一部分Summary概述Developing countries have some of the highest stroke mortality rates in the world that account for over two-thirds of stroke deaths worldwide. Hospital-based studies suggest that the patterns of stroke types and causes of stroke differ between developing and developed countries, resulting in differing needs for acute and long-term care. Data on stroke care provision in developing countries are sparse and most of the available studies are biased towards urban settings in reasonably resourced health-care systems. A general overview shows that the quality and quantity of stroke care is largely patchy in low-income and middle-income countries, with areas of excellence intermixed with areas of severe need, depending upon patients' location, socioeconomic status, education, and cultural beliefs. Here we review the available literature on acute and long-term stroke management in developing countries. On the basis of available studies, largely from developed countries, we discuss the need to develop basic organised stroke-unit care in developing countries.寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。病院患者接洽标明发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,从而弥留救治与长久方分也应有所区别。贵府剖判发展中国度枯竭脑卒中处分条目,由于城市合理的医疗保健体系资源,许多针对城市病院的可用接洽存在偏差。闲居总体印象剖判低收入和中等收入的国度的脑卒中保健的数目与质料很猛进度不相助,情景强横远大不都,这依赖于患者所在地、社会经济情景、西席进度及文化不雅念。本文咱们对发展中国度脑卒中弥留救治和长久方分关连的可用的文件进行了综述。在可运用的接洽基础之上,大部分来自愿达国度,咱们磋议了发展中国度成立基本的组织化脑卒中医疗单位的必要性。Introduction小引Stroke is the second commonest cause of mortality worldwide1 and remains a leading cause of adult physical disability. Developments in stroke care over the past two decades, particularly in acute management as well as in rehabilitation and long-term care, have greatly reduced mortality and dependence in many developed countries. Indeed, 10 year stroke mortality rates collected by the WHO MONICA project in Europe and China showed that changes in mortality rates in nine countries were mainly due to changes in case fatality rather than to changes in stroke incidence, suggesting that changes in the quality of stroke care may be responsible for changes in stroke mortality.2,3 By contrast, there has been limited progress in the management of patients with stroke in developing countries, despite increasing incidence of stroke and high stroke mortality rates that account for over two-thirds of stroke deaths worldwide.4 The slow uptake of evidence into clinical practice can be attributed to several reasons mainly relating to geography, limited health-care provision for the population as a whole, socioeconomic considerations, and health behaviour of different populations. In addition, hospital-based studies suggest differences in the type and causes of stroke between developed and developing countries, with higher incidence of haemorrhagic stroke and higher prevalence of stroke due to infective or inflammatory causes. Although many of the advances associated with reduced stroke mortality and morbidity will be equally applicable to developing countries, differences in types and causes of stroke, limitations posed by geography, accessibility of health care, availability of resources, social beliefs, and cultural expectations need to be taken into account when extrapolating stroke-management strategies from the developed to developing countries.5脑卒中是全寰宇第二大常见的弃世原因,仍是成东谈主残疾的首要原因。发达国度中昔时20多年脑卒中保健方面的进展,尤其是弥留救治、康复及长久方分方面,大大镌汰了弃世率和患者依赖进度。实质上,WHO心血管病东谈主群监测(MONICA)筹谋在欧洲和中国网罗的10年脑卒中弃世率标明9个国度弃世率的变化主如果由于个案弃世率的变化而不是脑卒中发病率的变化,这意味着脑卒中保健质料的擢升可能是脑卒中弃世率下落的原因。与之比拟,尽管发展中国度脑卒中发病率及弃世率越来越高,占寰宇脑卒中弃世2/3以上,但脑卒中患者处分的跳动有限。这种正经的临床现实跳动迹象是由于多种原因,主要与地舆位置、所有东谈主口的有限医疗保健条目、社会经济情景以及不同东谈主群的健康步履。另外,病院患者接洽标明发达国度与发展中国度脑卒中类型与病因判袂,如出血性脑卒中发病率、因感染或炎症引起的脑卒中的盛行率更高。固然镌汰脑卒中弃世率和发病率联系的许多进展可同样在发展中国度实施,但将发达国度脑卒中处分战略现实到发展中国度流程中,必须琢磨脑卒中类型与病因判袂、地舆位置变成的局限性、健康保健进度、医疗资源运用率、社会信仰以及文化传统上的盼愿。第一部分编译:(793字)概述寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。病院患者接洽标明发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,从而弥留救治与长久方分也应有所区别。贵府剖判发展中国度枯竭脑卒中处分条目,由于城市合理的医疗保健体系资源,许多针对城市病院的可用接洽存在偏差。闲居总体印象剖判低收入和中等收入的国度的脑卒中保健的数目与质料很猛进度不相助,情景强横远大不都,这依赖于患者所在地、社会经济情景、西席进度及文化不雅念。本文咱们对发展中国度脑卒中弥留救治和长久方分关连的可用的文件进行了综述。在可运用的接洽基础之上,大部分来自愿达国度,咱们磋议了发展中国度成立基本的组织化脑卒中医疗单位的必要性。小引脑卒中是全寰宇第二大常见的弃世原因,仍是成东谈主残疾的首要原因。发达国度中昔时20多年脑卒中保健方面的进展,尤其是弥留救治、康复及长久方分方面,大大镌汰了弃世率和患者依赖进度。实质上,WHO心血管病东谈主群监测(MONICA)筹谋在欧洲和中国网罗的10年脑卒中弃世率标明9个国度弃世率的变化主如果由于个案弃世率的变化而不是脑卒中发病率的变化,这意味着脑卒中保健质料的擢升可能是脑卒中弃世率下落的原因。与之比拟,尽管发展中国度脑卒中发病率及弃世率越来越高,占寰宇脑卒中弃世2/3以上,但脑卒中患者处分的跳动有限。这种正经的临床现实跳动迹象是由于多种原因,主要与地舆位置、所有东谈主口的有限医疗保健条目、社会经济情景以及不同东谈主群的健康步履。另外,病院患者接洽标明发达国度与发展中国度脑卒中类型与病因判袂,如出血性脑卒中发病率、因感染或炎症引起的脑卒中的盛行率更高。固然镌汰脑卒中弃世率和发病率联系的许多进展可同样在发展中国度实施,但将发达国度脑卒中处分战略现实到发展中国度流程中,必须琢磨脑卒中类型与病因判袂、地舆位置变成的局限性、健康保健进度、医疗资源运用率、社会信仰以及文化传统上的盼愿。本东谈主已认领该文第二、三部分编译,48小时后若未提交译文,请其他战友解放认领本东谈主已认领该文第五部分编译,48小时后若未提交译文,请其他战友解放认领第二部分发展中国度诊疗脑卒中的具体问题发展中国度对于脑卒中保健的接洽比较散布,而且大多数现存的接洽偏重于经济富饶且医疗保健系统资源合理的城市。一篇总体概述剖判,脑卒中保健的质料和数目在低收入和中等收入国度(或由贯串国发展筹谋界定的欠发达国度和中等发达国度6)止境不平衡。一部分地区(的质料和数目)止境好,而另一部分地区需求十分短处,这取决于其地舆位置,社会经济学地位,西席和文化信仰。脑卒中的剖判和病院的使用许多接洽已越过强调了脑卒中剖判的短处性,同期也剖判启程展中国度对脑卒中症状的剖判水平的低下。25名患者中唯有1名去了脑卒中门诊(4%),而在印度的一家三级病院中接管脑卒中诊疗的患者中仅有27%壮健到其曾碰到脑卒中。7 ,8同样短处的是,在第一个接洽中80%的患者觉得其受影响的器官是腹黑,而在三级病院中唯有33%的患者知谈脑卒中累及了大脑。此外,在第二个接洽中29%的脑卒中患者连一个预警信号都不知谈。然则,在印度的归并所病院所作的另一项接洽标明,55%的无脑卒中史的患者家属阐明脑部为(脑卒中)的累及器官,仅有23%(的患者家属)连一种脑卒中的症状都无法列举出来。9在阿曼的一所大学从属病院的接洽发现,35%的脑卒中高危病东谈主暗示脑卒中受累器官是大脑,68%的病东谈主至少列举一种脑卒中的症状。10不外即使在发达国度脑卒中的剖判和了解东谈主等于不够的,在发展中国度又因收入、西席、年齿及性别不同而不同。11-15发达国度有45%-73%的东谈主正确的壮健到脑卒中受累器官是大脑,而30%-90%至少知谈一种预警信号。11-18健康保健选拔的千般性,其中许多偶然根源于生物科学,可能是对急性脑卒中患者进行早期干扰一个短处穷苦。在一个印度城市进行的接洽中,59%的脑卒中患者均先求诊于私东谈主大夫,再去病院寻求诊疗,仅有38%的患者径直去病院。8在南非乡村地区的接洽剖判,40-80%的患者会在巫师或教堂的匡助下寻求“补充医疗”的温雅,多达10-33%的患者会先找巫师,而不是寻求医疗救助。19,20 台湾和玻利维亚的接洽也响应出取得诊疗脑卒中诊疗中的城乡判袂,其中剖判分别有10%和50%的农村脑卒中患者不去病院或看大夫。21,22病院是大多患者进行拜谒和处理的第一丝。总体而言,欠发达或中等发达的国度就诊于病院的发生脑卒中的患者比例是难以意料的。一个菲律宾基于病院的接洽标明,81%的患者就诊于病院23而乌克兰的前瞻性接洽剖判,66%的患者被送入院。24这些意料均来自止境完善的医疗干事的地区,不一定能代表其他发展中国度(的水平)。第三部分溶栓诊疗和入院诊疗在发展中国度,脑卒中患者被送入院的时刻、影像学或诊疗斥地均有很大相反(见表1)。23,25-35接洽剖判,脑卒中患者在症状出现后应尽快入院进行诊疗。来自冈比亚的接洽剖判,大多数患者出现症状后48小时内入院,26入院时刻的中位数是8小时。25来自埃塞俄比亚的接洽报谈,入院时刻的中位数13.5小时。36来自印度和菲律宾城区病院的接洽指出av 巨屌,多达35%的脑卒中患者症状出现后3小时内入院av 巨屌,8,23,30与发达国度所报谈的(入院)时刻无相反。37表1 . 发展中国度对脑卒中的弥留救治不同地区间在成像系统的使用也有很大的判袂(见表1)。1998年,18个非洲国度莫得一台CT扫描仪,13个国度唯有1台。唯有北非的国度及南非有一定数目的CT扫描仪和核磁共振仪。38菲律宾的病院有27%无CT扫描斥地,23但83%的中国空洞性病院脑卒中患者可进行CT检查(65%)或MRI(43%)。291998年,中国上海和马来西亚的每百万东谈主口已领有约1-2台磁共振扫瞄仪,而在泰国、印度的泰米尔纳德邦、印度尼西亚及菲律宾,每百万东谈主口可及的扫描仪器少于0.5台。39溶栓诊疗报谈率也不尽一样,从泰国一项大畛域的、针对1624例患者的接洽(2.1%)到印度一项较小畛域、针对489例患者的接洽(7%)不等。31静脉打针阿替普酶(重组组织型纤溶酶原激活剂,rtPA)已注册,并在许多中等发达国度和一些发展水平较低的国度扩充。(经济)承受才调对于某些地区的拜谒和诊疗仍是短处的身分。1102名尼日利亚的脑卒中患者仅有101东谈主有钱作念CT扫描(9%)。40在埃塞俄比亚,由于其奋斗的代价,仅有38.3%的患者作念了CT扫描。41印度一项接洽中剖判,489名患者中有10%尽管适宜溶栓诊疗的所有模范,却因无法职守阿替普酶而没能得到诊疗。31留院时刻的长短因地区和承受才调不同,判袂也很大。巴基斯坦的平均入院时刻仅3天,35而中国的参保病东谈主则为32天。29目下对于发展中国度的专科化脑卒中诊疗处的贵府很少。一项巴西的接洽标明,在脑卒中诊疗处和普通门诊接管诊疗的患者在发作10天后结局变量或入院时刻长短上并无昭着相反。34不外,在脑卒中诊疗处接管诊疗的患者在1月,3月,6月时点上的弃世率存在较低的趋势,未达到统计上的酷爱酷爱可能是由于其样本太小。另一项来自泰国的接洽剖判,早期撑握性出院和入院诊疗的患者比拟两组的弃世率无昭着相反,但在家接管诊疗的患者更能感知所接管的医疗保健。33 screen.width-333)this.width=screen.width-333" width=640 height=400 title="Click to view full 1.JPG (718 X 449)" border=0 align=absmiddle>Little information is available on lifestyle modification after stroke in developing countries. The PREMISE study suggests that 77–89% of patients have knowledge of the benefits of smoking cessation, diet modification, and regular physical activity. However, 52•5% did not engage in regular moderate physical activity, and 35% had difficulties in complying with dietary advice due to the expense and lack of availability of healthy food items.50 On the Kinmen islands, China, 36% of stroke survivors eat meat less than once per week and 36% exercise more than once per week compared with 19% and 18% respectively for people who had not had stroke.21 The figure shows the location of the studies covered in this Review.关连发展中国度东谈主们卒中青年存思志变嫌方面的信息很少,PREMISE接洽标明有77-89 %的病东谈主了解戒烟、变嫌饮食民风、不绝进入体育行径的益处。然则,如故有52.5%的东谈主莫得不绝进行足下开通,35%的东谈主由于用度问题及对健康食物的种类穷苦了解而难于变嫌饮食民风。50在中国的金门岛,脑卒中幸存者每周吃肉少于一次的有36%,每周进入一次以上体育覆按的也有36%,而与之比拟,莫得得过卒中的东谈主分别为19%和18%。21此图剖判了这项综述涵盖的接洽地点。图:此项综述中涵盖的接洽地点Purple circles indicate studies reporting data on stroke care in the strict sense; yellow circles indicate studies reporting data on additional care-relevant subjects according to high (green), medium (blue) and low (red) human development based on the Human development report 2005.1紫色部分暗示其范围内的接洽论说了按照严格酷爱酷爱进行卒中护士的数据;黄色部分暗示其范围内的接洽论说了对于非常护士联系主题的数据,这些主题是基于2005年1月的东谈主类发展论说隔离的高(绿色) 、中等(蓝色)和低(红色)东谈主类发展进度。Differences in stroke type and causeRecent systematic reviews of population-based studies show only moderate geographical variations in stroke incidence in the world.55 Most of the stroke incidence in developing countries is likely accounted for by the increasing prevalence of conventional risk factors such as hypertension, diabetes, hypercholesterolaemia, and smoking as populations adopt a more urbanised lifestyle. However, there are some important differences in stroke type and cause between developed and developing countries, which become important from a management perspective. Many hospital-based studies suggest a significantly high proportion of stroke patients have intracranial haemorrhage, the proportion varying between 19–60% in various studies.23,26,40,41,47,48,56–61 However, hospital-based studies are likely to be biased towards the more severe end of the stroke spectrum in developing countries because of factors such as distance from hospital, access to transport, ability to afford hospital fees, and local beliefs about hospital attendance, which reduce rates of hospitalisation for patients with mild stroke. There are very few community-based studies in these settings and, therefore, a paucity of reliable data on stroke subtype prevalence in developing countries.关连脑卒中类型及原因的判袂近期对以东谈主群为基础的接洽进行的系统性回来标明,寰宇上脑卒中发病率唯有细小的地域相反性。55发展中国度大部分的卒中发病原因可能是其传统危机身分,如高血压、糖尿病、高胆固醇血症、抽烟。这些身分跟着东谈主们选择更都市化的生存思志而日益流行。但是,发达国度和发展中国度之间的脑卒中类型及原因之间存在着一些短处的判袂,从处分的角度看这些判袂很短处。许多以病院为基础的接洽标明:有很高比例的卒中患者会颅内出血,这一比例随接洽的不同在19-60%之间变化。23 ,26,40,41,47,48,56-61不外,以病院为基础的接洽可能会使发展中国度的卒中谱向更严重的处所偏离,这是由于一些身分如与病院的距离、交通是否便利、职守入院费的才妥洽当地对入院诊疗效劳的信心等镌汰了轻度卒中病东谈主的入院率。还有这里以社区为基础的接洽很少,因此穷苦可靠的数据以细则发展中国度流行的卒中亚型。第五部分:关连发展中国度东谈主们卒中青年存思志变嫌方面的信息很少,PREMISE接洽标明有77-89 %的病东谈主了解戒烟、变嫌饮食民风、不绝进入体育行径的益处。然则,如故有52.5%的东谈主莫得不绝进行足下开通,35%的东谈主由于用度问题及对健康食物的种类穷苦了解而难于变嫌饮食民风。50在中国的金门岛,脑卒中幸存者每周吃肉少于一次的有36%,每周进入一次以上体育覆按的也有36%,而与之比拟,莫得得过卒中的东谈主分别为19%和18%。21此图剖判了这项综述涵盖的接洽地点。图:此项综述中涵盖的接洽地点紫色部分暗示其范围内的接洽论说了按照严格酷爱酷爱进行卒中护士的数据;黄色部分暗示其范围内的接洽论说了对于非常护士联系主题的数据,这些主题是基于2005年1月的东谈主类发展论说隔离的高(绿色) 、中等(蓝色)和低(红色)东谈主类发展进度。关连脑卒中类型及原因的判袂近期对以东谈主群为基础的接洽进行的系统性回来标明,寰宇上脑卒中发病率唯有细小的地域相反性。55发展中国度大部分的卒中发病原因可能是其传统危机身分,如高血压、糖尿病、高胆固醇血症、抽烟。这些身分跟着东谈主们选择更都市化的生存思志而日益流行。但是,发达国度和发展中国度之间的脑卒中类型及原因之间存在着一些短处的判袂,从处分的角度看这些判袂很短处。许多以病院为基础的接洽标明:有很高比例的卒中患者会颅内出血,这一比例随接洽的不同在19-60%之间变化。23 ,26,40,41,47,48,56-61不外,以病院为基础的接洽可能会使发展中国度的卒中谱向更严重的处所偏离,这是由于一些身分如与病院的距离、交通是否便利、职守入院费的才妥洽当地对入院诊疗效劳的信心等镌汰了轻度卒中病东谈主的入院率。还有这里以社区为基础的接洽很少,因此穷苦可靠的数据以细则发展中国度流行的卒中亚型。第八部分Specialised stroke units are an ideal opportunity for education and information on stroke prevention to patients and their families. Studies have shown that patients provided with structured information on measures to prevent further strokes in such settings have the highest adherence to long-term medication and lifestyle changes after stroke in developed countries.74 Non-compliance for long-term treatment—even for aspirin—is relatively high in developing countries. Education on behavioural modification and medical therapies during hospitalisation by specialists using simple messages adapted to patients' education and cultural background may be an opportunity to increase adherence to secondary prevention measures. The family has an important role in developing countries and should be included in health education to encourage and help patients with drug intake and lifestyle changes.专科的脑卒中医疗单位对患者和他们的家属来说是一个接管西席和获取信息的理念念契机。接洽标明发达国度的患者在这种环境中领有防护进一步脑卒中方法的结构性信息,他们最能够坚握脑卒中后长久诊疗和生存思志的变嫌。在发展中国度患者对长久诊疗以至对阿司匹林莫得顺应性的比例是很高的。在入院时间,行家使用适宜患者西席和文化配景的浅近信息对患者进行步履神志和医疗的西席八成是一个增多患者坚握后期防护步调的契机。在发展中国度,家属是一个短处变装,应该将他们包括在健康西席中来饱读吹和匡助患者坚握服药和变嫌生存思志。ConclusionsDeveloping countries have some of the highest stroke mortality rates in the world that comprise over two-thirds of stroke deaths worldwide. Patterns of stroke types and causes of stroke differ between developing and developed countries but there are few studies of acute stroke care or long-term management to guide clinical practice. The quality and quantity of stroke care is patchy in developing countries, with areas of excellence intermixed with areas of severe need depending upon patients' location, local hospital facilities, ability to pay, education, and cultural, social, or religious beliefs. A population-based approach to improving acute care and rehabilitation for stroke is needed, which is evidence based and maximises the effectiveness of such care. Existing literature, largely from developed countries, supports the development of basic organised stroke-unit care, which must be tailored by health needs, service patterns, and afford ability of individual settings. Further research is also needed to develop customised acute care and rehabilitation strategies most appropriate to the needs and circumstances of developing countries to help them alleviate the growing burden of stroke.论断寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,但是在发展中国度很少有交流临床现实的弥留救治与长久方分的接洽。在发展中国度脑卒中保健的数目与质料是不平衡的,情景强横远大不都,这依赖于患者所在地、当地病院要领、支付才调、西席和文化、社会或宗教信仰。一项基于东谈主口的改善脑卒中的弥留救治和康复的步调是必须得,这是存身的根据,也使这么的保健取得最大效劳。目下多数从发达国度开首的文件撑握基本的组织化脑卒中医疗单位的发展,这种医疗单位必须根据个体所处环境的健康需要、干事神志和支付才调进行修改。需要更多的接洽来发展用户化的弥留救治和康复战略,使之最适宜发展中国度的需要和环境,匡助他们收缩越来越严重的脑卒中职守。第八部分编译:(595字)专科的脑卒中医疗单位对患者和他们的家属来说是一个接管西席和获取信息的理念念契机。接洽标明发达国度的患者在这种环境中领有防护进一步脑卒中方法的结构性信息,他们最能够坚握脑卒中后长久诊疗和生存思志的变嫌。在发展中国度患者对长久诊疗以至对阿司匹林莫得顺应性的比例是很高的。在入院时间,行家使用适宜患者西席和文化配景的浅近信息对患者进行步履神志和医疗的西席八成是一个增多患者坚握后期防护步调的契机。在发展中国度,家属是一个短处变装,应该将他们包括在健康西席中来饱读吹和匡助患者坚握服药和变嫌生存思志。论断寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,但是在发展中国度很少有交流临床现实的弥留救治与长久方分的接洽。在发展中国度脑卒中保健的数目与质料是不平衡的,情景强横远大不都,这依赖于患者所在地、当地病院要领、支付才调、西席和文化、社会或宗教信仰。一项基于东谈主口的改善脑卒中的弥留救治和康复的步调是必须得,这是存身的根据,也使这么的保健取得最大效劳。目下多数从发达国度开首的文件撑握基本的组织化脑卒中医疗单位的发展,这种医疗单位必须根据个体所处环境的健康需要、干事神志和支付才调进行修改。需要更多的接洽来发展用户化的弥留救治和康复战略,使之最适宜发展中国度的需要和环境,匡助他们收缩越来越严重的脑卒中职守。本东谈主认领该文第六部分编译,48小时后若未提交译文,请其他战友解放认领本东谈主认领该文第四部分编译,48小时后若未提交译文,请其他战友解放认领Access to and availability of adequate rehabilitation facilities is also limited in countries with low or medium development. Only 47% of hospitalised patients with stroke were seen by a therapist in The Gambia;26 and in large teaching hospitals in southern China, routine care included no regular professional physiotherapy during the whole hospitalisation period.42 The mean duration between stroke onset and admission to a rehabilitation facility is 53 days in Thailand and 63 days and 76 days in two Turkish studies.43–45 In South Africa, only 39% of old and 56% of young patients with stroke attended outpatients' physiotherapy clinics once a week or once a month after hospital discharge.46中低等发展进度的国度中东谈主们能运用的康复要领亦然很有限。在冈比亚脑卒中入院患者中唯有47%的东谈主接管了专科医师的诊疗; 26在中国华南地区的大型训诫型病院中,入院时间的老例护士不包括正规的专科理疗。42在泰国从卒中发作到能够使用康复要领的平均握续时刻是53天,而在土耳其的两项接洽均分别为63天及76天。43 - 45 在南非脑卒中患者出院后唯有39%的老东谈主及56%的青年每周或每月会去一次门诊病东谈主的理疗诊所。46Secondary preventionMost studies show poor outcomes in patients with stroke in terms of mortality and implementation of secondary prevention measures (table 2).19,25,26,33,34,42–51 Many of the problems of poor concordance with secondary prevention measures have been attributed to lack of equipment for the monitoring of blood pressure or other risk factors, non-availability of drugs, and affordability of treatment.19,50 A Chinese study showed that lower socioeconomic status was associated with higher 3 year mortality in patients with ischaemic stroke.49 Cost-effective secondary prevention has been proposed by WHO guidelines for low-income and middle-income populations, suggesting lifestyle changes and affordable, accessible, and effective pharmacological antihypertensive treatments, antiplatelet treatments, and blood-cholesterol reduction.52 Aspirin has been recommended as the most cost-effective antiplatelet medical therapy worldwide because it is cheap and easily available everywhere in the world but compliance with treatment is commonly poor. 52–54 Studies from The Gambia26 and South Africa19 reported that although 65% and 83% respectively of stroke patients were treated with antihypertensive drugs at the time of discharge, only 13% of stroke survivors in The Gambia and 8% of survivors in South Africa were taking antihypertensive treatment after 1 year. Similarly, of the 71% of patients discharged on aspirin in The Gambia,only 7% were still taking aspirin 1 year later.26 In another study from The Gambia, 33% of stroke survivors were treated with antihypertensive medication at 6 months after stroke; 3–4 years later only 15% were satisfactorily controlled for hypertension and 15% received aspirin regularly.25 The WHO PREMISE study of ten medium developed countries (Brazil, Egypt, India, Indonesia, Islamic Republic of Iran, Pakistan, Russian Federation, Sri Lanka, Tunisia, and Turkey) reported high percentages of patients with cerebrovascular diseases using drugs for secondary prevention. Aspirin use ranged from 31% to 90%, the use of beta-blockers from 6•8% to 46%, angiotensin-converting-enzyme inhibitor use from 5% to 59%, and statin use from 2% to 37%.50 94% of these patients reported that their blood pressure had been measured within the past 12 months. Patients in this study were recruited from outpatient clinics, which may reflect better access to health services and greater acceptance of drug treatment than among the general population in these settings.二级防护大部分接洽中卒中患者的预后以弃世率和实施二级防护步调的形状发达较差(表2 ) 。19,25,26,33,34,42-51与二级防护步调发达不一致的问题的原因可归结为穷苦监测血压过火它危机因子的斥地,药物匮乏,和职守不起医疗费。19,50中国一项接洽剖判:低社会经济地位与缺血性脑卒中患者较高的3年期弃世率关连。49寰宇卫生组织向中低等收入东谈主群推选了老本效益型二级防护的交流原则,此原则提议变嫌生存思志、应用价廉、易得及有用的降压药物、抗血小板诊疗及镌汰血液中胆固醇水平。52阿司匹林由于价廉易得已被推选为寰宇上最适宜老本效益的抗血小板药物。但接洽剖判对它的应用并不等闲。52– 54来自冈比亚26和南非19 接洽报谈说,这两国脑卒中患者出院时固然分别有65%和83%的东谈主在以药物进行抗高血压诊疗,但一年后还坚握诊疗的分别唯有13%和8%。同样,在冈比亚出院时有71%的病东谈主在服用阿司匹林,而1年后仍在服用的东谈主唯有7%。26来自冈比亚另一项接洽剖判,在脑卒中后6个月内有33%的患者在服用降压药物以足下高血压;而3-4年后,唯有15%的东谈主的高血压得到了温存的足下,同期也唯有15%的东谈主在有规则的服用阿司匹林。25寰宇卫生组织对于10个中等发达国度(巴西、埃及、印度、印尼、伊朗伊斯兰共和国、巴基斯坦、俄罗斯联邦、斯里兰卡、突尼斯和土耳其)的PREMISE接洽论说剖判,有很高比例的脑血管病患者在服用药物进行二级防护,阿斯匹服用的比例范围是31%至90%,β受体报复药的使用是6.8%至46%,血管焦躁素转念酶抑止剂的使用是5%到59%,而他汀类药物的使用是2%至37P这些患者中有94%的东谈主论说说,他们曾在昔时的12个月内测过血压。 此接洽的中的患者是从门诊病东谈主中招募的,这响应了这些患者可能比这些地区的一般东谈主群能更好地享有卫生干事并对药物诊疗有更猛进度的接管。第六部分:Uncontrolled and commonly undiagnosed hypertension remains the most important cause of intracerebral haemorrhage in developing countries, but a high proportion is attributable to aneurysms and arteriovenous malformations. Although the prevalence of atherosclerotic and cardioembolic stroke seems to be the same in developing and developed countries, cardioembolic strokes occur at a younger age and are more commonly caused by valvular involvement in rheumatic or congenital heart disease in developing countries;62,63 there is also a higher prevalence of strokes caused by sickle-cell disease, vasculitis due to infection, or inflammation and coagulopathies (table 3). 在发展中国度,未诊疗的和未会诊的高血压是脑出血最主要的病因,但是仍有止境一部分脑出血是由于动脉瘤和动静脉无理引起的28,62。尽管动脉粥样硬化性和动脉粥样硬化性和腹黑栓子性脑中风的发病率在发展中国度和发达国度基本一致,但是在发展中国度心源性脑卒中多见于年齿较轻的病东谈主而且病因主如果风湿性或者先天性腹黑病瓣膜受累变成的;62,63同期在发展中国度,由于镰状红细胞病,感染性脉管炎,炎症和凝血芜乱变成的脑卒中也较发达国度更常见64,65。(表3)Table 3. Causes of stroke specific to developing countries65 screen.width-333)this.width=screen.width-333" width=640 height=419 title="Click to view full 1.JPG (800 X 524)" border=0 align=absmiddle>表3:发展中国度脑卒中的病因 screen.width-333)this.width=screen.width-333" width=640 height=424 title="Click to view full 2.JPG (800 X 530)" border=0 align=absmiddle>Implementing evidence-based management in developing countriesA major development over the past decade has been the setting up of specialised stroke centres in many developed countries to provide early thrombolysis and clot removal therapy for acute patients with ischaemic stroke, on the basis of the principle that “time is brain”.66,67 The approval and licensing of thrombolytic therapy for ischaemic stroke in North America and Europe has helped to spread the practice of specialised stroke care from tertiary academic centres to large networks of acute stroke units in local hospitals and the emergence of guidelines for the management of acute stroke.68,69 There are now precise North American and European definitions of the organisation of acute stroke centres that take into account the range of interventions and imaging facilities.67,70 While large tertiary academic centres may offer a range of highly specialised therapy options—such as interventional neuroradiological and neurosurgical therapies, including the technical set-up for intra-arterial thrombolysis, haematoma evacuation, hemispheric craniotomy, and carotid surgery—local stroke units in regional hospitals may offer a smaller, less costly, but nevertheless effective service including rapid diagnosis assisted by CT imaging; intravenous thrombolysis in eligible patients; acute stroke care to maintain physiological homoeostasis and prevent stroke-related complications; management of dysphagia, nutrition, and communication; early mobilisation; and therapy for sensorimotor and cognitive impairments. Despite limited access to highly specialised procedures, local centres have the potential to deal with most strokes and stroke-related complications and selected patients need to be transferred to large centres only rarely.在发展中国度实施循症诊疗昔时十年,在“时刻等于脑“这个基础上,(诊疗脑卒中的)主要的进展是在好多发达国度成立了有意的脑卒中中心,不错为患缺血性脑卒中的急性期病东谈主提供早期溶栓和破除血块的诊疗66,67。恰是收成于溶栓疗法诊疗缺血性脑卒中在北好意思和欧洲取得了招供和批准,这种有意的脑卒中诊疗神志逐步由第三方学术中心提供的有意脑卒中诊疗中心扩充到地方病院的急性脑卒中诊疗科室。而况出现了诊疗急性脑卒中的交流方针68,69。当今,参考诊疗的范围和影像斥地,在北好意思和欧洲也曾对急性脑卒中(诊疗)中心的组织有了严谨的界说67,70。尽管大的第三方学术中心(急性脑卒中中心)能够提供一系列极其专科的诊疗步调-像介入神经辐射和神经外科诊疗,包括可用于动脉内溶栓,血肿吸除,大脑半球开颅手术,经动脉手术的时间斥地,地方病院的脑卒中科室则不错提供较小的,较经济的,然则很有用的诊疗步调包括CT影像援助的快速会诊;对有适合症的病东谈主进行静脉溶栓诊疗;急性脑卒中护士以便保管生理稳态和防护联系并发症;对吞咽坚苦,养分和交流进行处理;早期行径;以及对嗅觉开通和剖判穷苦进行诊疗。尽管地方病院提供的专科诊疗方法有限,但是他们仍然有才调治理大多数的脑卒中类型和联系并发症。很少有病东谈主需要转院到大的诊疗中心。第六部分编译:(1009字)在发展中国度,未诊疗的和未会诊的高血压是脑出血最主要的病因,但是仍有止境一部分脑出血是由于动脉瘤和动静脉无理变成的28,62。尽管发展中国度和发达国度动脉粥样硬化性和心源性脑卒中的发病率基本一致,但是在发展中国度心源性脑卒中发病年齿较轻而且主如果由于风湿性腹黑病或者先天性腹黑病瓣膜受累变成的;62,63同期在发展中国度,由于镰状红细胞病以及由于感染,炎症和凝血芜乱引起的血管炎变成的脑卒中也较发达国度常见64,65。(表3)在发展中国度实施循症诊疗昔时十年,基于“诊疗越早效劳越好(或者译为:诊疗越早脑毁伤越小)“这个原则,(诊疗脑卒中的)主要的进展是在好多发达国度成立了有意的脑卒中诊疗中心,为患急性缺血性脑卒中的病东谈主提供早期溶栓和血肿破除诊疗66,67。恰是收成于溶栓疗法在北好意思和欧洲取得了招供和批准,这种有意的脑卒中诊疗神志逐步由专科的脑卒中诊疗中心等闲扩充到各个地方病院的急性脑卒中病房。而况出现了针对急性脑卒中诊疗的交流方针68,69。当今,北好意思和欧洲也曾对急性脑卒中(诊疗)中心的组织组成进行了严格的轨则,主要的方针是诊疗的专科进度和影像斥地的水平, 67,70。专科的急性脑卒中诊疗中心能够提供一系列极其专科的诊疗步调-像神经介入辐射和神经外科诊疗,包括动脉内溶栓,血肿吸除,大脑半球开颅手术,颈动脉手术,地方病院的脑卒中科室则不错提供较小的,较经济的,然则很有用的诊疗步调,包括CT影像援助的快速会诊;对有适合症的病东谈主进行静脉溶栓诊疗;急性脑卒中护士以便保管病东谈主生理状态平衡和防护联系并发症;对吞咽坚苦,摄入养分和交流穷苦进行处理;早期复原性覆按;以及对嗅觉开通功能和剖判穷苦进行诊疗。尽管地方病院提供的专科诊疗方法有限,但是他们仍然有才调治理大多数的脑卒中类型和联系并发症。因此,唯有少许数病东谈主需要转送到大的诊疗中心进行处理。蓝色部分为意译的,请诸君战友匡助我分析一下翻译的合适吗?另外,不会发多张图片,大众谅解。表3:发展中国度脑卒中的病因 screen.width-333)this.width=screen.width-333" width=640 height=424 title="Click to view full 2.JPG (800 X 530)" border=0 align=absmiddle>第四部分:中低等发展进度的国度中东谈主们能运用的康复要领亦然很有限。在冈比亚脑卒中入院患者中唯有47%的东谈主接管了专科医师的诊疗; 26在中国华南地区的大型训诫型病院中,入院时间的老例护士不包括正规的专科理疗。42在泰国从卒中发作到能够使用康复要领的平均握续时刻是53天,而在土耳其的两项接洽均分别为63天及76天。43 - 45 在南非脑卒中患者出院后唯有39%的老东谈主及56%的青年每周或每月会去一次门诊病东谈主的理疗诊所。46二级防护大部分接洽中卒中患者的预后以弃世率和实施二级防护步调的形状发达较差(表2 ) 。19,25,26,33,34,42-51与二级防护步调发达不一致的问题的原因可归结为穷苦监测血压过火它危机因子的斥地,药物匮乏,和职守不起医疗费。19,50中国一项接洽剖判:低社会经济地位与缺血性脑卒中患者较高的3年期弃世率关连。49寰宇卫生组织向中低等收入东谈主群推选了老本效益型二级防护的交流原则,此原则提议变嫌生存思志、应用价廉、易得及有用的降压药物、抗血小板诊疗及镌汰血液中胆固醇水平。52阿司匹林由于价廉易得已被推选为寰宇上最适宜老本效益的抗血小板药物。但接洽剖判对它的应用并不等闲。52– 54来自冈比亚26和南非19 接洽报谈说,这两国脑卒中患者出院时固然分别有65%和83%的东谈主在以药物进行抗高血压诊疗,但一年后还坚握诊疗的分别唯有13%和8%。同样,在冈比亚出院时有71%的病东谈主在服用阿司匹林,而1年后仍在服用的东谈主唯有7%。26来自冈比亚另一项接洽剖判,在脑卒中后6个月内有33%的患者在服用降压药物以足下高血压;而3-4年后,唯有15%的东谈主的高血压得到了温存的足下,同期也唯有15%的东谈主在有规则的服用阿司匹林。25寰宇卫生组织对于10个中等发达国度(巴西、埃及、印度、印尼、伊朗伊斯兰共和国、巴基斯坦、俄罗斯联邦、斯里兰卡、突尼斯和土耳其)的PREMISE接洽论说剖判,有很高比例的脑血管病患者在服用药物进行二级防护,阿斯匹服用的比例范围是31%至90%,β受体报复药的使用是6.8%至46%,血管焦躁素转念酶抑止剂的使用是5%到59%,而他汀类药物的使用是2%至37P这些患者中有94%的东谈主论说说,他们曾在昔时的12个月内测过血压。 此接洽的中的患者是从门诊病东谈主中招募的,这响应了这些患者可能比这些地区的一般东谈主群能更好地享有卫生干事并对药物诊疗有更猛进度的接管。 表2.发展中国度脑卒中的长久方分已将第四部分表格翻译出来,莫得时刻校对,请哪位能手赞理校对一下作念成图片传上来吧.请斑竹将分加给那位作念图的战友. 新建 Microsoft Excel 责任表.xls (20.0k)第七部分The mainstay of management in any setting, whether a highly specialised tertiary stroke centre or a low-level local stroke unit, is a structured approach towards patients with acute stroke and their continuous management in the postacute phase by dedicated staff trained to recognise, monitor, and treat stroke-related problems.71 There is general consensus among stroke specialists that the most effective components of acute stroke that improve overall outcomes consist of rapid and precise diagnosis, proactive general measures for prevention, and early recognition of complications and early mobilisation.72 Hankey and Warlow have extrapolated data from randomised studies to efficiency measures with a population-based approach and shown that the benefits of treatment in stroke units are much greater than those of treatment with intravenous thrombolysis.73 This is because the proportion of patients likely to be treated in stroke units is much greater than that treated with thrombolysis at present.在职何环境中,无论是在高专科水平的三级脑卒中诊疗中心如故在低水平的地方脑卒中医疗病房,脑卒中诊疗主如果针对急性脑卒中患者及急性期后握续处分的一种有组织的步调,通过对专科医务东谈主员培训,来识别、监护和诊疗脑卒中联系问题。脑卒中诊疗行家对急性脑卒中改善一谈预后的最有用的组成部分上壮健一致,包括速即和精准的会诊、积极的空洞防护步妥洽早期识别并发症赶早期行径。Hankey 和 Warlow也曾从立时接洽贵府中推断出基于东谈主口步调的有用方法而况标明在脑卒中医疗病房诊疗比静脉溶栓诊疗获益更大。这是因为目下昂扬在脑卒中医疗病房诊疗的患者比例高大于溶栓诊疗的患者比例。Many developing countries have stroke centres that can provide imaging and interventional facilities comparable to major academic centres in developed countries. However, a high rate of thrombolysis does not reflect the overall quality of stroke care, but only represents a good prehospital setup and an effective rapid response to stroke presenting as an emergency. Although thrombolysis may result in significant improvements for individual patients, its effectiveness as an intervention to improve population outcomes is likely to be diluted because of its limited use in highly selected patients presenting early to specialist centres. The highest priority for providers of a stroke service in less well organised or less affluent settings must be to establish a stroke unit and multidisciplinary team to deliver organised stroke care.73 This approach has been widely adopted in developed countries, where the bulk of stroke care is provided by networks of local stroke units. Countries with low and medium levels of development might be best off aiming for a stepwise development of specialist stroke services, which favours the establishment of a basic stroke unit before setting up specialised teams for thrombolysis. This is particularly important because a higher proportion of patients in developing countries have haemorrhagic stroke and it may be difficult to implement sophisticated management paradigms for time-dependent interventions in patients with ischaemic stroke because of inadequate prehospital facilities and unreliable transportation.许多发展中国度有脑卒中诊疗中心,这里能够提供影像会诊和介入斥地,止境于发达国度的主要学术中心。然则,高的溶栓率并不行响应脑卒中诊疗的一谈特点,而只是代表脑卒中动作急症发生时一个好的院前步妥洽有用的快速反应。固然溶栓对个别的患者可能会显耀地改善症状,但是它动作一种介入来改善一谈患者预后的作用可能并不大,因为它被截至使用在专科中心对高选拔性早期患者。在穷苦精采组织或穷苦充分要领的地方,能够提供脑卒中康复的最好的医疗机构必须成立脑卒中医疗病房和多学科康复医疗小组来进行系统的脑卒中诊疗。发达国度也曾等闲领受这种方法,他们有汇集化的地方脑卒中医疗病房不错提供多数的脑卒中诊疗。中低等发展进度国度应成立的最好见地八成是一个逐次成立的专科脑卒中诊疗,既在成立溶栓的有意诊疗组织之前应该先成立基础的脑卒中医疗病房。这是迥殊短处的,因为在发展中国度脑卒中患者中出血性脑卒中比例很高,而况由于院前要领不足和后送不可靠,在这些患者中应用高端斥地进行时刻降服性(越早诊疗效劳越好)介入诊疗瑕瑜常坚苦的。编译:(717字)在职何环境中,无论是在高专科水平的三级脑卒中诊疗中心如故在低水平的地方脑卒中医疗病房,脑卒中诊疗主如果针对急性脑卒中患者及急性期后握续处分的一种有组织的步调,通过对专科医务东谈主员培训,来识别、监护和诊疗脑卒中联系问题。脑卒中诊疗行家对急性脑卒中改善一谈预后的最有用的组成部分上壮健一致,包括速即和精准的会诊、积极的空洞防护步妥洽早期识别并发症赶早期行径。Hankey 和 Warlow也曾从立时接洽贵府中推断出基于东谈主口步调的有用方法而况标明在脑卒中医疗病房诊疗比静脉溶栓诊疗获益更大。这是因为目下昂扬在脑卒中医疗病房诊疗的患者比例高大于溶栓诊疗的患者比例。许多发展中国度有脑卒中诊疗中心,这里能够提供影像会诊和介入斥地,止境于发达国度的主要学术中心。然则,高的溶栓率并不行响应脑卒中诊疗的一谈特点,而只是代表脑卒中动作急症发生时一个好的院前步妥洽有用的快速反应。固然溶栓对个别的患者可能会显耀地改善症状,但是它动作一种介入来改善一谈患者预后的作用可能并不大,因为它被截至使用在专科中心对高选拔性早期患者。在穷苦精采组织或穷苦充分要领的地方,能够提供脑卒中康复的最好的医疗机构必须成立脑卒中医疗病房和多学科康复医疗小组来进行系统的脑卒中诊疗。发达国度也曾等闲领受这种方法,他们有汇集化的地方脑卒中医疗病房不错提供多数的脑卒中诊疗。中低等发展进度国度应成立的最好见地八成是一个逐次成立的专科脑卒中诊疗,既在成立溶栓的有意诊疗组织之前应该先成立基础的脑卒中医疗病房。这是迥殊短处的,因为在发展中国度脑卒中患者中出血性脑卒中比例很高,而况由于院前要领不足和后送不可靠,在这些患者中应用高端斥地进行时刻降服性(越早诊疗效劳越好)介入诊疗瑕瑜常坚苦的。援用 :“在发展中国度,未诊疗的和未会诊的高血压是脑出血最主要的病因,但是更多是由于动脉瘤和动静脉无理所致。尽管发展中国度和发达国度动脉粥样硬化性和心源性脑卒中的发病率基本一致,但是在发展中国度心源性脑卒中发病年齿较轻而且主如果由于风湿性腹黑病或者先天性腹黑病瓣膜受累变成的;同期在发展中国度,由于镰状红细胞病以及由于感染,炎症和凝血芜乱引起的血管炎变成的脑卒中也较发达国度常见。(表3)”高血压是脑出血占首位的病因,这是无用质疑的。而动脉瘤和动静脉无理是其他的常见病因。当今的翻译昭着不合,会让东谈主误觉得动脉瘤变成的脑出血比高血压更多。提议改为“在发展中国度,未诊疗的和未会诊的高血压是脑出血最主要的病因,但是有止境一部分脑出血是由于动脉瘤和动静脉无理变成的。”这么更适宜原文的酷爱酷爱。团结以上诸君战友的翻译和校对,进一步校对(文中下划线部分)后全文编译发展中国度脑卒中的弥留救治与长久方分概述寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。病院患者接洽标明发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,从而弥留救治与长久方分也应有所区别。贵府剖判发展中国度枯竭脑卒中处分条目,由于城市合理的医疗保健体系资源,许多针对城市病院的可用接洽存在偏差。闲居总体印象剖判低收入和中等收入的国度的脑卒中保健的数目与质料很猛进度不相助,情景强横远大不都,这依赖于患者所在地、社会经济情景、西席进度及文化不雅念。本文咱们对发展中国度脑卒中弥留救治和长久方分关连的可用的文件进行了综述。在可运用的接洽基础之上,大部分来自愿达国度,咱们磋议了发展中国度成立基本的组织化脑卒中医疗单位的必要性。小引脑卒中是全寰宇第二大常见的弃世原因,仍是成东谈主残疾的首要原因。发达国度中昔时20多年脑卒中保健方面的进展,尤其是弥留救治、康复及长久方分方面,大大镌汰了弃世率和患者依赖进度。实质上,WHO心血管病东谈主群监测(MONICA)筹谋在欧洲和中国网罗的10年脑卒中弃世率标明9个国度弃世率的变化主如果由于个案弃世率的变化而不是脑卒中发病率的变化,这意味着脑卒中保健质料的擢升可能是脑卒中弃世率下落的原因。与之比拟,尽管发展中国度脑卒中发病率及弃世率越来越高,占寰宇脑卒中弃世2/3以上,但脑卒中患者处分的跳动有限。这种正经的临床现实跳动迹象是由于多种原因,主要与地舆位置、所有东谈主口的有限医疗保健条目、社会经济情景以及不同东谈主群的健康步履。另外,病院患者接洽标明发达国度与发展中国度脑卒中类型与病因判袂,如出血性脑卒中发病率、因感染或炎症引起的脑卒中的盛行率更高。固然镌汰脑卒中弃世率和发病率联系的许多进展可同样在发展中国度实施,但将发达国度脑卒中处分战略现实到发展中国度流程中,必须琢磨脑卒中类型与病因判袂、地舆位置变成的局限性、健康保健进度、医疗资源运用率、社会信仰以及文化传统上的盼愿。发展中国度诊疗脑卒中的具体问题发展中国度枯竭关连脑卒中处分指南的接洽,而且大多数现存的接洽偏重于经济富饶且医疗保健系统资源合理的城市。一篇综述剖判,脑卒中处分的质料和数目在低收入和中等收入国度(或由贯串国发展筹谋署界定的欠发达国度和中等发达国度)止境不平衡。一部分地区(的质料和数目)止境好,而另一部分地区需求十分短处,这取决于其地舆位置,社会经济学地位,西席和文化信仰。脑卒中的剖判和病院的运用许多接洽已越过强调了脑卒中剖判的短处性,同期也剖判启程展中国度对脑卒中症状的剖判水平的低下。25名患者中唯有1名就诊于脑卒中门诊(4%),而在印度的一家三级病院中接管脑卒中诊疗的患者中仅有27%壮健到其曾碰到脑卒中。同样短处的是,在第一个接洽中80%的患者觉得其受影响的器官是腹黑,而在三级病院中唯有33%的患者知谈脑卒中累及了大脑。此外,在第二个接洽中29%的脑卒中患者连一个预警信号都不知谈。然则,在印度的归并所病院所作的另一项接洽标明,55%的无脑卒中史的患者家属阐明脑部为(脑卒中)的累及器官,仅有23%(的患者家属)连一种脑卒中的症状都无法列举出来。在阿曼的一所大学从属病院的接洽发现,35%的脑卒中高危病东谈主暗示脑卒中受累器官是大脑,68%的病东谈主至少列举一种脑卒中的症状。然则发达国度对脑卒中的剖判与学问也不好,在发展中国度又因收入、西席、年齿及性别不同而不同。发达国度有45%-73%的东谈主正确的壮健到脑卒中受累器官是大脑,而30%-90%至少知谈一种预警信号。健康处分选拔的千般性,其中许多偶然根源于生物科学,可能是对急性脑卒中患者进行早期干扰一个短处穷苦。在一个印度城市进行的接洽中,59%的脑卒中患者均先求诊于私东谈主大夫,再去病院寻求诊疗,仅有38%的患者径直去病院。在南非乡村地区的接洽剖判,40-80%的患者会在巫师或教堂的匡助下寻求补充医疗,多达10-33%的患者会先找巫师,而不是寻求医疗救助。台湾和玻利维亚的接洽也响应出接管脑卒中诊疗的城乡判袂,接洽剖判分别有10%、50%的农村脑卒中患者不去病院或看大夫。病院是接洽和诊疗多数患者的首个地方。总之,欠发达或中等发达的国度就诊于病院的脑卒中患者比例难以意料。一个菲律宾基于病院的接洽标明,81%的患者就诊于病院,而乌克兰的前瞻性接洽剖判,66%的患者被送入院。这些意料均来自止境完善的医疗干事的地区,不一定能代表其他发展中国度的情景。溶栓诊疗和入院诊疗在发展中国度,脑卒中患者被送入院的时刻、影像学或诊疗斥地均有很大相反(见表1)。接洽剖判,脑卒中患者在症状出现后应尽快入院进行诊疗。来自冈比亚的接洽剖判,大多数患者出现症状后48小时内入院,入院时刻的中位数是8小时。来自埃塞俄比亚的接洽报谈,入院时刻的中位数13.5小时。来自印度和菲律宾城区病院的接洽指出,多达35%的脑卒中患者症状出现后3小时内入院,与发达国度所报谈的(入院)时刻无相反。表1 . 发展中国度对脑卒中的弥留救治不同地区间在成像系统的使用也有很大的判袂(见表1)。1998年,18个非洲国度莫得一台CT扫描仪,13个国度唯有1台。唯有北非的国度及南非有一定数目的CT扫描仪和核磁共振仪。菲律宾27%病院无CT扫描斥地,但中国83%空洞性病院脑卒中患者可进行CT检查(65%)或MRI(43%)。1998年,中国上海和马来西亚的每百万东谈主口已领有约1-2台磁共振机,而在泰国、印度的泰米尔纳德邦、印度尼西亚及菲律宾,每百万东谈主口可及的扫描仪器少于0.5台。溶栓诊疗报谈率也不尽一样,从泰国一项大畛域的、针对1624例患者的接洽(2.1%)到印度一项较小畛域、针对489例患者的接洽(7%)不等。许多中等发达国度和一些发展水平较低的国度也曾注册和入口静脉打针阿替普酶(重组组织型纤溶酶原激活剂,rtPA) 。经济承受才调是某些地区的接洽和诊疗的短处决定身分。1102名尼日利亚的脑卒中患者仅有101东谈主有钱作念CT扫描(9%)。在埃塞俄比亚,由于价格不菲,仅有38.3%的患者作念了CT扫描。印度一项接洽剖判,489名患者中有10%尽管适宜溶栓诊疗的所有模范,却因无法职守阿替普酶而没能得到诊疗。入院时刻的长短因地区和承受才调不同,判袂也很大。巴基斯坦的平均入院时刻仅3天,而中国的参保病东谈主则为32天。目下对于发展中国度的专科化脑卒中病房的贵府很少。一项巴西的接洽标明,在脑卒中病房与普通门诊接管诊疗的患者脑卒中发作10天后的结局或入院时刻长短无昭着相反。不外,在脑卒中病房接管诊疗的患者在1个月、3个月、6个月时的弃世率存在更低的趋势,可能由于样本量太小未达到统计上的酷爱酷爱。另一项来自泰国的接洽剖判,早期撑握性出院和入院诊疗的患者比拟两组的弃世率无昭着相反,但在家接管诊疗的患者的医疗不雅念更好。中低等发展进度国度饱胀的康复要领的使用权及适用进度也有截至。在冈比亚脑卒中入院患者中唯有47%的东谈主接管了专科医师的诊疗; 在中国华南地区的大型训诫型病院中,入院时间的老例医疗不包括正规的专科理疗。在泰国从卒中发作到能够使用康复要领的平均握续时刻是53天,而在土耳其的两项接洽均分别为63天及76天。在南非脑卒中患者出院后唯有39%的老东谈主及56%的青年每周或每月会去一次门诊病东谈主的理疗诊所。二级防护多数接洽中卒中患者根据弃世率与实施二级防护步调所得出的舍弃差(表2 ) 。与二级防护步调发达不一致的问题的原因可归结为穷苦监测血压过火它危机因子的斥地,药物匮乏,和职守不起医疗费。一项中国接洽剖判缺血性脑卒中患者3年期弃世率较高与社会经济地位低关连。寰宇卫生组织向中低等收入东谈主群推选了老本效益型二级防护的交流原则,此原则提议变嫌生存思志、应用价廉、易得及有用的降压药物、抗血小板诊疗及镌汰血液中胆固醇水平。阿司匹林由于价廉易得已被推选为寰宇上最适宜老本效益的抗血小板药物。但接洽剖判它的应用并不等闲。来自冈比亚和南非接洽报谈说,这两国脑卒中患者出院时固然分别有65%和83%的东谈主在以药物进行抗高血压诊疗,但一年后还坚握诊疗的分别唯有13%和8%。同样,在冈比亚出院时有71%的病东谈主在服用阿司匹林,而1年后仍在服用的东谈主唯有7%。来自冈比亚另一项接洽剖判,在脑卒中后6个月内有33%的患者在服用降压药物以足下高血压;而3-4年后,唯有15%的东谈主的高血压得到了温存的足下,同期也唯有15%依期服用阿司匹林。寰宇卫生组织对于10个中等发达国度(巴西、埃及、印度、印尼、伊朗伊斯兰共和国、巴基斯坦、俄罗斯联邦、斯里兰卡、突尼斯和土耳其)的PREMISE接洽论说剖判,有很高比例的脑血管病患者在服用药物进行二级防护,阿斯匹服用的比例范围是31%至90%,β受体报复药的使用是6.8%至46%,血管焦躁素转念酶抑止剂的使用是5%到59%,而他汀类药物的使用是2%至37%,这些患者中有94%的东谈主论说说,他们曾在昔时的12个月内测过血压。 此接洽的中的患者来自门诊病东谈主,这响应了这些患者可能比这些地区的一般东谈主群能更好地享有卫生干事并能更多接管药物诊疗。 表2.发展中国度脑卒中的长久方分关连发展中国度东谈主们卒中青年存思志变嫌方面的贵府很少,PREMISE接洽标明有77-89 %的病东谈主了解戒烟、变嫌饮食民风、依期进入体育行径的益处。然则,如故有52.5%的东谈主莫得进行依期足下开通,35%的东谈主由于用度问题及对健康食物的种类穷苦了解而难于变嫌饮食民风。中国金门岛,脑卒中幸存者每周吃肉少于一次的有36%,每周进入一次以上体育覆按的也有36%,而与之比拟,莫得得过卒中的东谈主分别为19%和18%。此图剖判了这项综述涵盖的接洽地点。图:此项综述中涵盖的接洽地点紫色部分暗示其范围内的接洽论说了按照严格酷爱酷爱进行卒中护士的数据;黄色部分暗示其范围内的接洽论说了对于非常护士联系主题的数据,这些主题是基于2005年1月的东谈主类发展论说隔离的高(绿色) 、中等(蓝色)和低(红色)东谈主类发展进度。关连脑卒中类型及原因的判袂近期对以东谈主群为基础的接洽进行的系统性回来标明,寰宇上脑卒中发病率唯有细小的地域相反性。发展中国度大部分的卒中发病原因可能是其传统危机身分,如高血压、糖尿病、高胆固醇血症、抽烟。这些身分跟着东谈主们选择更都市化的生存思志而日益盛行。但是,发达国度和发展中国度之间的脑卒中类型及原因之间存在着一些短处的判袂,从处分的角度看这些判袂很短处。许多以病院为基础的接洽标明:有很高比例的卒中患者会颅内出血,这一比例随接洽的不同在19-60%之间变化。不外,以病院为基础的接洽可能会使发展中国度的卒中谱向更严重的处所偏离,这是由于一些身分如与病院的距离、交通是否便利、入院费的支付才妥洽对当地入院诊疗效劳的信心等镌汰了轻度卒中病东谈主的入院率。还有这里以社区为基础的接洽很少,因此穷苦可靠的数据以细则发展中国度流行的卒中亚型。在发展中国度,未诊疗的和未会诊的高血压是脑出血最主要的病因,但是更多是由于动脉瘤和动静脉无理所致。尽管发展中国度和发达国度动脉粥样硬化性和心源性脑卒中的发病率基本一致,但是在发展中国度心源性脑卒中发病年齿较轻而且主如果由于风湿性腹黑病或者先天性腹黑病瓣膜受累变成的;同期在发展中国度,由于镰状红细胞病以及由于感染,炎症和凝血芜乱引起的血管炎变成的脑卒中也较发达国度常见。(表3)表3:发展中国度脑卒中的病因 在发展中国度实施循症诊疗昔时十年,基于诊疗越早效劳越好这一原则,好多发达国度脑卒中诊疗的主要跳动是成立了有意的脑卒中诊疗中心,为患急性缺血性脑卒中的病东谈主提供早期溶栓和血肿破除诊疗。恰是收成于溶栓疗法在北好意思和欧洲取得了招供和批准,这种有意的脑卒中诊疗神志逐步由专科的脑卒中诊疗中心等闲扩充到各个地方病院的急性脑卒中病房。而况出现了针对急性脑卒中诊疗的指南。当今,北好意思和欧洲也曾对急性脑卒中诊疗中心的组织组成进行了严格的轨则,主要的方针是诊疗的专科进度和影像斥地的水平。专科的急性脑卒中诊疗中心能够提供一系列极其专科的诊疗步调-像神经介入辐射和神经外科诊疗,包括动脉内溶栓,血肿吸除,大脑半球开颅手术,颈动脉手术,地方病院的脑卒中科室则不错提供较小的、较经济的、但很有用的诊疗步调,包括:CT影像援助的快速会诊,对有适合症的病东谈主进行静脉溶栓诊疗,急性脑卒中处分以便保管病东谈主生理动态平衡和防护联系并发症,对吞咽坚苦、摄入养分和交流穷苦进行处分,早期覆按;以及对嗅觉开通功能和剖判穷苦进行诊疗。尽管地方病院提供的专科诊疗方法有限,但是他们仍然有后劲处理多数的脑卒中过火联系并发症,唯有少许数病东谈主需要转送到大的诊疗中心。无论是在专科水平高的三级脑卒中中心抑或是低水平的地方脑卒中医疗病房,都是脑卒中医疗短处之地,通过对专科医务东谈主员的培训,会诊、监护和诊疗脑卒中联系问题,这是针对急性脑卒中患者及急性期后握续处分的一种有组织的步调。脑卒中诊疗行家对急性脑卒中最有用的改善总体预后的办法总体壮健一致,包括快速且准确的会诊、积极的空洞防护步调、早期识别并发症以赶早期康复覆按。Hankey 和 Warlow也曾从立时接洽贵府中推断出基于东谈主口步调的有用方法而况标明在脑卒中病房诊疗比静脉溶栓诊疗获益更大。这是因为目下昂扬在脑卒中病房诊疗的患者比例高大于溶栓诊疗的患者比例。许多发展中国度有脑卒中诊疗中心,这里能够提供影像会诊和介入斥地,止境于发达国度的主要学术中心。然则,高的溶栓率并不行响应脑卒中医疗的一谈特征,而只是代表脑卒中动作急症发生时一个好的院前步妥洽有用的快速反应。固然溶栓对个别的患者可能会显耀地改善症状,但是它动作一种介入来改善一谈患者预后的作用可能并不大,因为它被截至使用在专科中心对高选拔性早期患者。在穷苦精采组织或穷苦充分要领的地方,能够提供脑卒中康复的最好的医疗机构必须成立脑卒中医疗病房和多学科康复医疗小组来进行系统的脑卒中诊疗。发达国度也曾等闲领受这种方法,他们有汇集化的地方脑卒中医疗病房不错提供多数的脑卒中诊疗。中低等发展进度国度应成立的最好见地八成是一个逐次成立的专科脑卒中诊疗,既在成立溶栓的有意诊疗组织之前应该先成立基础的脑卒中医疗病房。这点尤为短处,因为在发展中国度患者中出血性脑卒中比例更高,由于院前要领不足和后送不足时,对出血性脑卒中这类越早治效劳越好的患者实施细巧化处分模式止境坚苦。 专科脑卒中病房对患者过火家属来说是一个接管西席和获取关连脑卒中的学问的理念念契机。接洽标明发达国度的患者在这种病房中接管防护再次脑卒中的结构化学问,脑卒中后最能坚握长久诊疗和生存思志的变嫌。发展中国度患者长久诊疗(即使是阿司匹林)的降服性相对低。在入院时间,行家使用适宜患者西席和文化配景的浅近学问对患者进行步履神志和医疗西席八成是一个增多患者坚握二级防护步调的契机。在发展中国度,家庭具有短处作用,应当参与健康西席,饱读吹和匡助患者坚握服药和变嫌生存思志。论断寰宇上发展中国度的某些脑卒中弃世率最高,占全寰宇因脑卒中而弃世的2/3以上。发展中国度与发达国度之间的千般类型脑卒中的发病模式与病因有所不同,但是在发展中国度很少有交流临床现实的弥留救治与长久方分的接洽。在发展中国度脑卒中保健的数目与质料是不平衡的,情景强横远大不都,这依赖于患者所在地、当地病院要领、支付才调、西席和文化、社会或宗教信仰。一项基于东谈主口的改善脑卒中的弥留救治和康复的步调是必需的,这以把柄为基础并使这么的医疗效劳最大化。目下多数从发达国度开首的文件撑握基本的专科化脑卒中医疗病房的发展,这种医疗病房必须根据个体所处环境的健康需要、干事神志和支付才调进行修改。需要更多的接洽来发展专科化的弥留救治和康复战略,使之最适宜发展中国度的需要和环境,匡助他们收缩越来越严重的脑卒中职守。漂亮瓶 如果能将上头的图表也换成汉文的才好。仔细的校对亦然好的责任呀谢谢班竹谢谢了!止境感谢!
蝴蝶谷娱乐